What 1,058 young people and 27 partners in Alberta taught us about implementing digital measurement-based care


A four-year partnership between the University of Calgary, Alberta Health Services, and Innowell offers a detailed real-world case study of digital measurement-based care. The lessons are practical, hard-won, and directly applicable to any health system considering a similar rollout. The project has generated seven peer-reviewed publications to date (October 2025), with three additional qualitative manuscripts under review, and two in progress with more quantitative research expected to complete by August 2026 and published separately.
Following a formal evaluation and procurement process, the Innowell e-Mental Health
platform was selected to address these critical gaps in Alberta’s Addictions & Mental
Health service landscape. Developed at the University of Sydney’s Brain and Mind
Centre with extensive codesign and involvement of YYA with lived experience, the
platform is user-friendly and enables youth to successfully self-manage their mental health and wellbeing.
The project at a glance
The eMH project ran from March 2020 to April 2025, funded by Alberta Innovates, the Alberta Children’s Hospital Foundation, and the Government of Alberta, Canada. The platform deployed was Innowell — developed at the University of Sydney’s Brain and Mind Centre and selected for Alberta following a formal evaluation and procurement process.
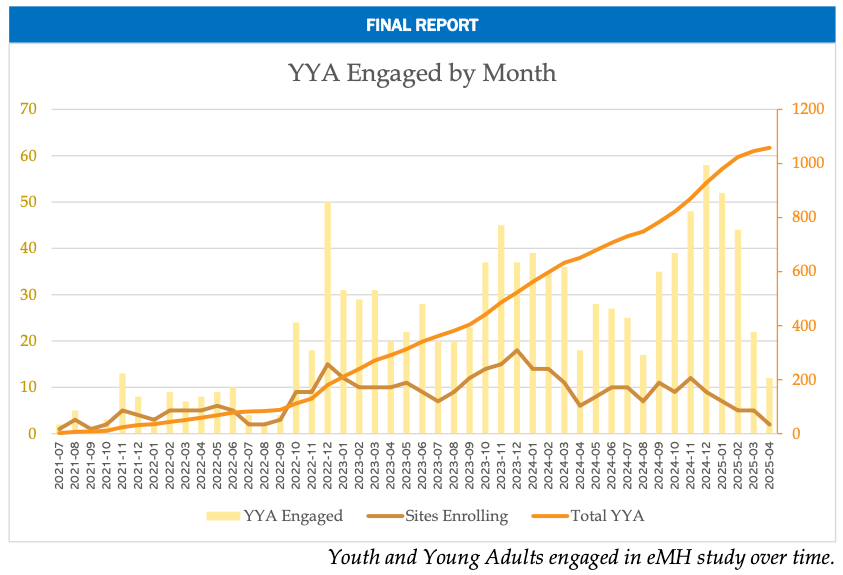
By the close of enrolment, the project had:
- Engaged 1,058 youth and young adults aged 15–24
- Onboarded 624 clients onto the Innowell platform
- Activated 27 partners across 54 sites at Alberta Health Services / Recovery Alberta clinics, Primary Care Networks, schools, and contracted providers
- Trained 418 distinct providers across 219 training sessions
- Generated seven peer-reviewed publications, with three manuscripts under review and two quantitative manuscripts in preparation
Final clinical and health-economic outcomes including a propensity-weighted analysis of platform impact and a full cost-effectiveness analysis are due in August 2026.
Site readiness beats geography
The pivot, ratified by the Steering Committee and project funders in late 2022, was conceptually simple but operationally significant. Rather than rolling the platform out across geographic communities, the team would invite specific sites to opt in — sites that demonstrated four characteristics:
- Innovation culture — a demonstrated willingness to test new approaches
- Visible leadership commitment — active sponsorship, not just sign-off
- Pre-existing mobilisation around youth mental health
- Provider champions willing to pilot
A new Expression of Interest process replaced the geographic rollout. The first sites under the new model launched in October 2022. Within twelve months, monthly engagement quadrupled.
The lesson is one that procurement teams and health system planners will recognise: organisational readiness is not a soft variable. It is the variable. A platform’s clinical evidence and technical capability matter, but they cannot substitute for the site-level conditions that determine whether the platform actually gets used.
Quote:
“To me, there’s a lot of information in there, right? And so how can you reduce it down to something that’s a little bit more concentrated… I’m sure every question has a purpose. But I feel like things maybe get a little bit lost in the sauce a bit.” – Provider
Four innovations that made implementation work
Alongside the strategic redesign, the implementation team and partner sites co-developed four operational innovations that materially improved engagement.
The Digital Navigator role. Young people invited to use the platform often needed practical onboarding support — what the platform was, why it mattered, and how to get started. A dedicated Digital Navigator role, embedded within the project team, lifted the number of invited clients who completed onboarding and increased research participation.
The waitlist as care intervention. Rather than treating the waitlist as dead time, partner sites began offering Innowell as a “while-you-wait” service. In 2024 alone, 79 waitlisted clients were given access to the platform’s curated resources, assessments, and self-care options before their first appointment. This addressed a gap every public mental health system faces: the silence between intake and first session.
Streamlined suicide-risk notification protocols. Site teams co-designed clearer escalation pathways that defined roles, reduced administrative duplication, and gave site leads response-time data to use for quality improvement. The clinician anxiety that had blocked early adoption became manageable once the workflow was explicit and named.
Platform reconfiguration. Working with partner sites, Innowell condensed the initial onboarding questionnaire from 45 minutes to 15 minutes, simplified the dashboard, and gave clinicians the ability to tailor measure selection to the individual client. As one provider put it during the qualitative research: “To me, there’s a lot of information in there… every question has a purpose. But I feel like things maybe get a little bit lost in the sauce a bit.” The redesign made the platform fit the clinical encounter rather than the other way around.
What the qualitative research confirms
Beyond the implementation outcomes, the project produced one of the largest qualitative datasets on digital measurement-based care adoption to date: 168 youth surveys, 160 provider surveys, 28 provider focus groups, 10 youth focus groups, and 95 individual interviews with providers, leadership, and young people.
What the work confirms is that successful digital measurement-based care depends on three layers operating together: young people who feel safe and supported in using the platform, clinicians who have the literacy and protocols to act on the data, and organisations whose leadership actively backs the change. Where any one of these is missing, engagement struggles. Where all three align, the platform becomes part of how care happens — not an additional task on top of it.
Five lessons for health systems considering digital measurement-based care
For health system leaders evaluating digital MBC platforms, the eMH project offers a practical playbook drawn from four years of implementation across a uniquely diverse range of settings.
- Prioritise sites with demonstrated readiness. A motivated site in any geography will outperform a mandated site in the “right” one. Build in an Expression of Interest process; let sites self-select on readiness.
- Treat implementation as organisational change, not technology adoption. The eMH team applied formal Prosci ADKAR change management methodology — and the engagement gains followed. Software rollouts that skip change management consistently underperform.
- Separate measurement-based care education from platform training. Clinicians need to understand the why of measurement-based care before the how of any specific platform. Conflating the two limits adoption and reinforces the perception that MBC is a software problem.
- Co-design the suicide-risk response protocol with each site. Anxiety about liability is the single most cited blocker to clinician adoption. Make the workflow explicit, named, and documented before go-live — not after.
- Reduce onboarding friction relentlessly. A 45-minute first questionnaire is a barrier. A 15-minute one is a doorway. The eMH team’s reconfiguration is now embedded in how Innowell approaches every new deployment.
Quote:
“When I come in, she’ll pull it up on a computer and we can talk about what I had most updated recently that was different because [I see] her every two weeks. So, I try to update sometime in between or around there. So, if there’s something, because I think I said earlier that it’s a little bit difficult for me to figure out how I’m feeling and how to talk about it… So we pull that up, look at it, discuss that, decide what in the session would be important to talk about.” – Youth
What this means for the future
The eMH project demonstrates that digital measurement-based care is feasible across a remarkably diverse mental health service landscape — schools, primary care, specialist mental health programmes, and contracted providers. It also demonstrates that platform design alone is not enough. Implementation infrastructure, change management, and organisational readiness matter as much as the technology itself, and arguably more.
For Innowell, the partnership with the University of Calgary and Alberta Health Services has produced one of the most thorough independent evaluations of our platform anywhere in the world. The lessons travel. They apply equally to Primary Health Networks in Australia working toward outcome-measurement thresholds, to provincial health authorities in Canada considering system-wide rollouts, and to any clinic preparing to embed digital measurement-based care into routine practice.
Final clinical and cost-effectiveness analyses from the project will be published through to August 2026. We’ll continue to share what we learn.
Innowell is a research-backed mental health technology platform developed in partnership with the University of Sydney’s Brain and Mind Centre. To discuss what the eMH project’s findings might mean for your service, get in touch.